
When Repetitive Habits in Autism Cross the Line Into OCD — And Why It Matters
You check the stove three times before leaving the house. You replay a conversation in your head for an hour. You need your morning routine to happen in exactly the same order, every single day, or the whole day feels "off."
For most people, these habits are quirks. But for someone on the autism spectrum, they can be part of a much bigger question — one that even doctors find challenging to answer: Is this just how my brain works, or is this OCD?
The answer matters more than you might think. It changes what kind of help actually works — and what kind of help might make things worse.
Two Conditions That Look Alike on the Surface
Autism spectrum disorder (ASD) and obsessive-compulsive disorder (OCD) can both involve repetitive thoughts and behaviors. But beneath the surface, they are driven by very different engines.
Think of it this way:
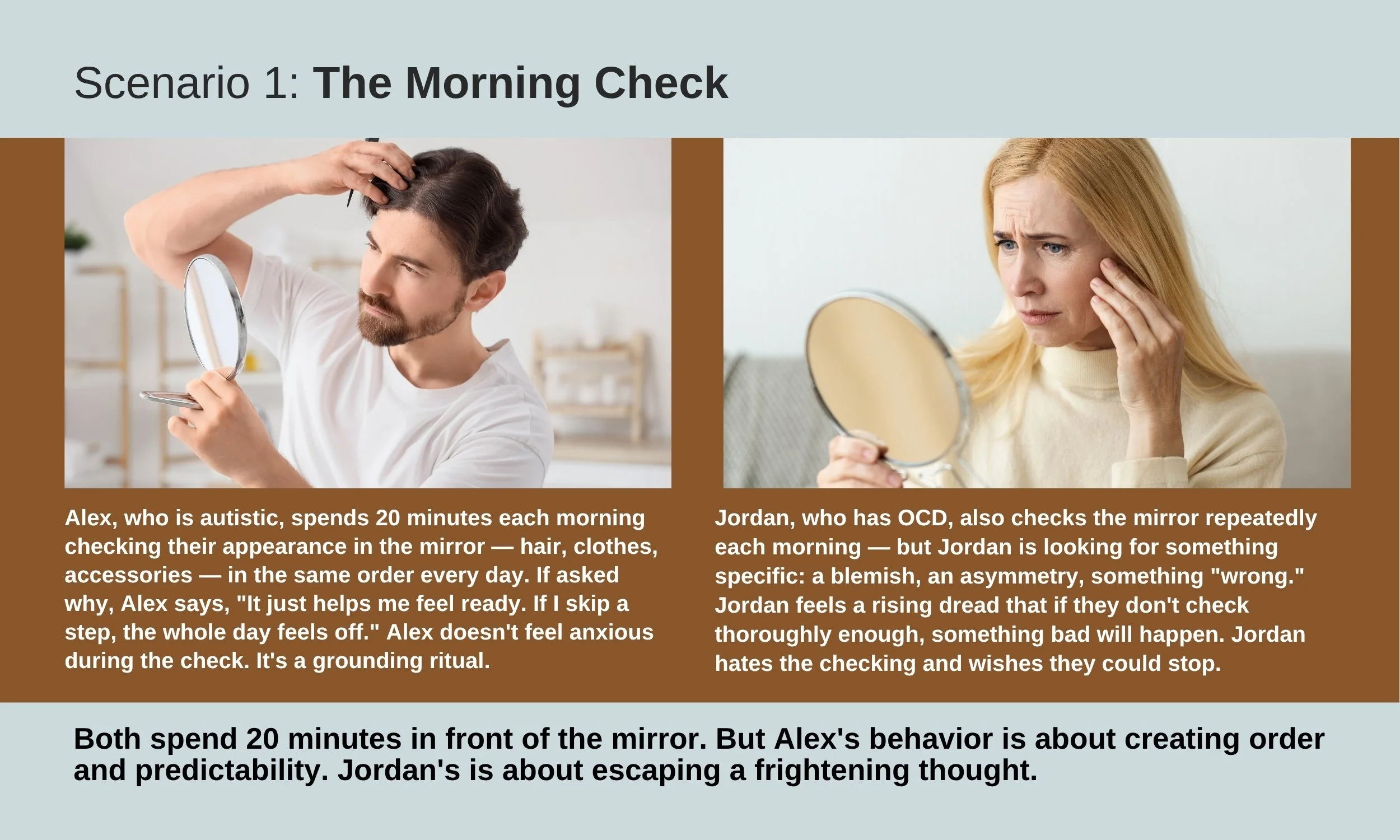
A person with OCD who washes their hands repeatedly does so because they are haunted by the thought that they might get sick or contaminate someone. They don't want to wash — they feel they have to. The handwashing is an attempt to escape a frightening thought.
An autistic person who follows a rigid morning routine — shower, then coffee, then checking their bag in a specific order — does so because the routine itself feels stabilizing. It creates a sense of order and predictability. They aren't trying to escape a scary thought. The routine just feels right, and breaking it feels deeply uncomfortable.
Same behavior on the outside. Completely different experience on the inside.
Why This Isn't Just an Academic Distinction
This matters because the treatments that work for OCD can actually backfire when applied to autism-related habits — and vice versa.
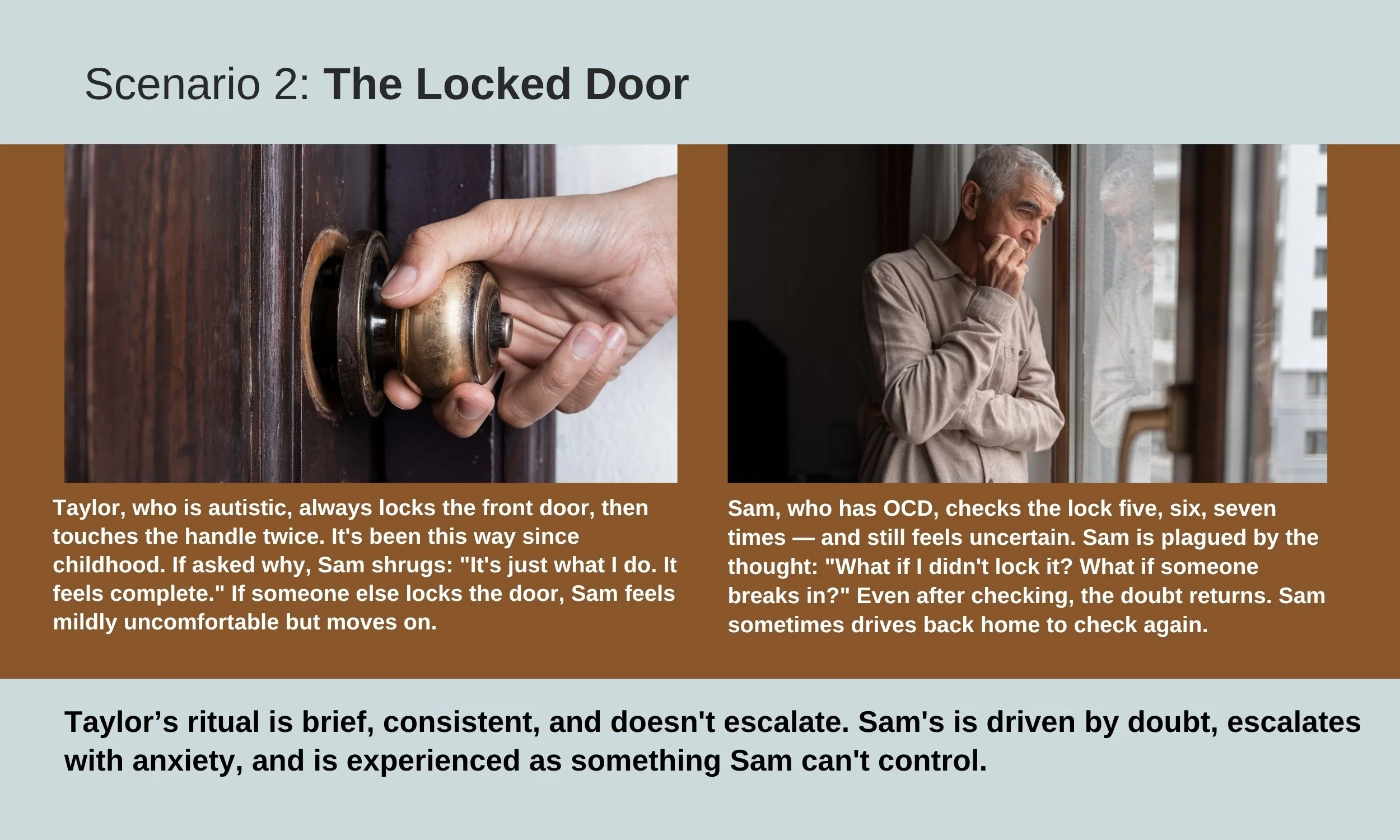
The gold-standard therapy for OCD is called Exposure and Response Prevention (ERP). It works by gradually exposing a person to the thing that triggers their anxiety (say, touching a doorknob) and then helping them resist the urge to perform the compulsion (not washing their hands). Over time, the anxiety fades on its own. It's highly effective — for OCD.
But if a person's repetitive behavior is serving as a calming, regulating function — as it often does in autism — then forcing them to stop it doesn't reduce anxiety. It creates distress without any therapeutic benefit. It's like taking away someone's noise-canceling headphones in a loud room and expecting them to feel better.
Similarly, medications called SSRIs (like fluoxetine or sertraline) are a cornerstone of OCD treatment. But research consistently shows that these same medications have little effect on autism-related repetitive behaviors. Prescribing an SSRI for a behavior that looks like OCD but is actually an autism trait means side effects without benefit.
The Overlap Is Real — and Common
Here's what makes this even more complicated: many autistic people do also have OCD. Studies suggest that roughly 1 in 5 autistic adults may meet the criteria for OCD — far higher than the roughly 1 in 50 rate in the general population. And the relationship goes both ways: people diagnosed with OCD are about four times more likely to also be on the autism spectrum.
So the question isn't always "Is this autism or OCD?" Sometimes it's "Is this autism and OCD?" — and figuring out which behaviors belong to which condition is essential for getting the right help.
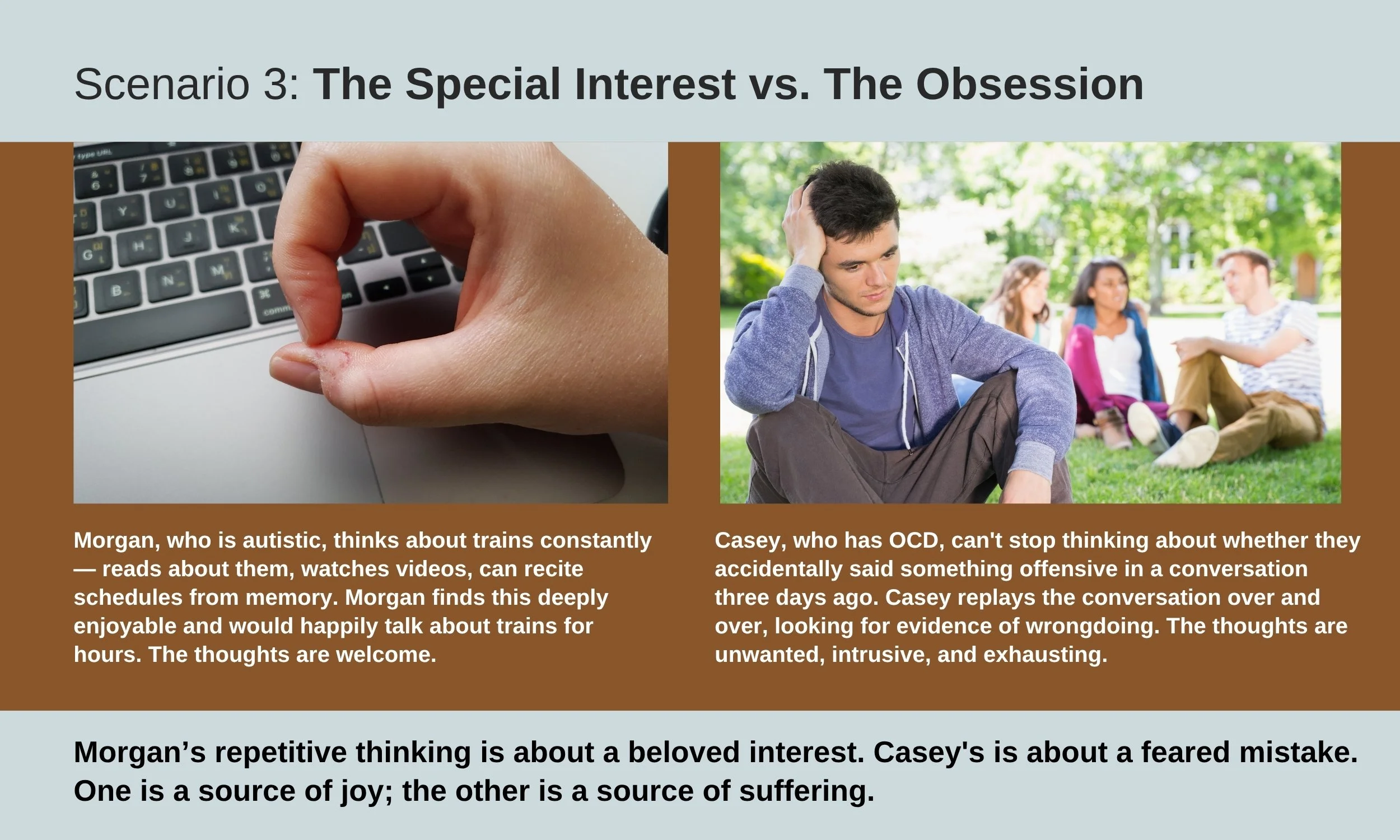
How to Tell the Difference: Real-Life Examples
Here are some everyday scenarios that illustrate the distinction:
When It Gets Tricky
These examples make the distinction sound clear-cut. In real life, it often isn't. Here's why:
Many autistic people have difficulty naming their emotions. This is called alexithymia, and it's common in autism. When a healthcare provider asks, "Does this thought cause you anxiety?", an autistic person with alexithymia might say "no" — not because they aren't distressed, but because they can't easily label what they're feeling. Or they might say "yes" because any strong internal sensation gets called "anxiety" by default. This makes the standard clinical interview unreliable without careful adaptation.
Distress upon interruption isn't the same as OCD anxiety. If you interrupt an autistic person's routine and they become very upset, that doesn't mean the routine was driven by OCD. The distress comes from the disruption of predictability — not from an intrusive, threatening thought. It's the difference between someone being upset because you rearranged their desk (a predictability issue) and someone being upset because they believe something terrible will happen if the desk isn't arranged a certain way (an OCD issue).
The same person can have both. An autistic person might have a comforting morning routine (autism) and also experience intrusive, unwanted thoughts about contamination that drive compulsive handwashing (OCD). The morning routine should be respected and accommodated. The handwashing should be treated. A skilled clinician can help distinguish which is which.
What the Brain Science Tells Us
Researchers have found that although both autism and OCD involve some of the same brain circuits — particularly the loops connecting the front of the brain (which handles planning and decision-making) to deeper structures (which handle habits and routines) — the pattern of dysfunction is actually opposite:
In OCD, these circuits are overactive — like a car engine revving too high. The brain's habit system is in overdrive, generating compulsive behaviors that the thinking brain can't shut down.
In autism, these same circuits are wired differently from the start — not overactive, but developed along a different path. The repetitive behaviors aren't a malfunction of the habit system; they're a feature of how the brain organized itself.
This is why the same medication that calms the overactive OCD circuit (an SSRI) doesn't have the same effect on the differently-wired autism circuit. They look similar from the outside, but the underlying biology is different.
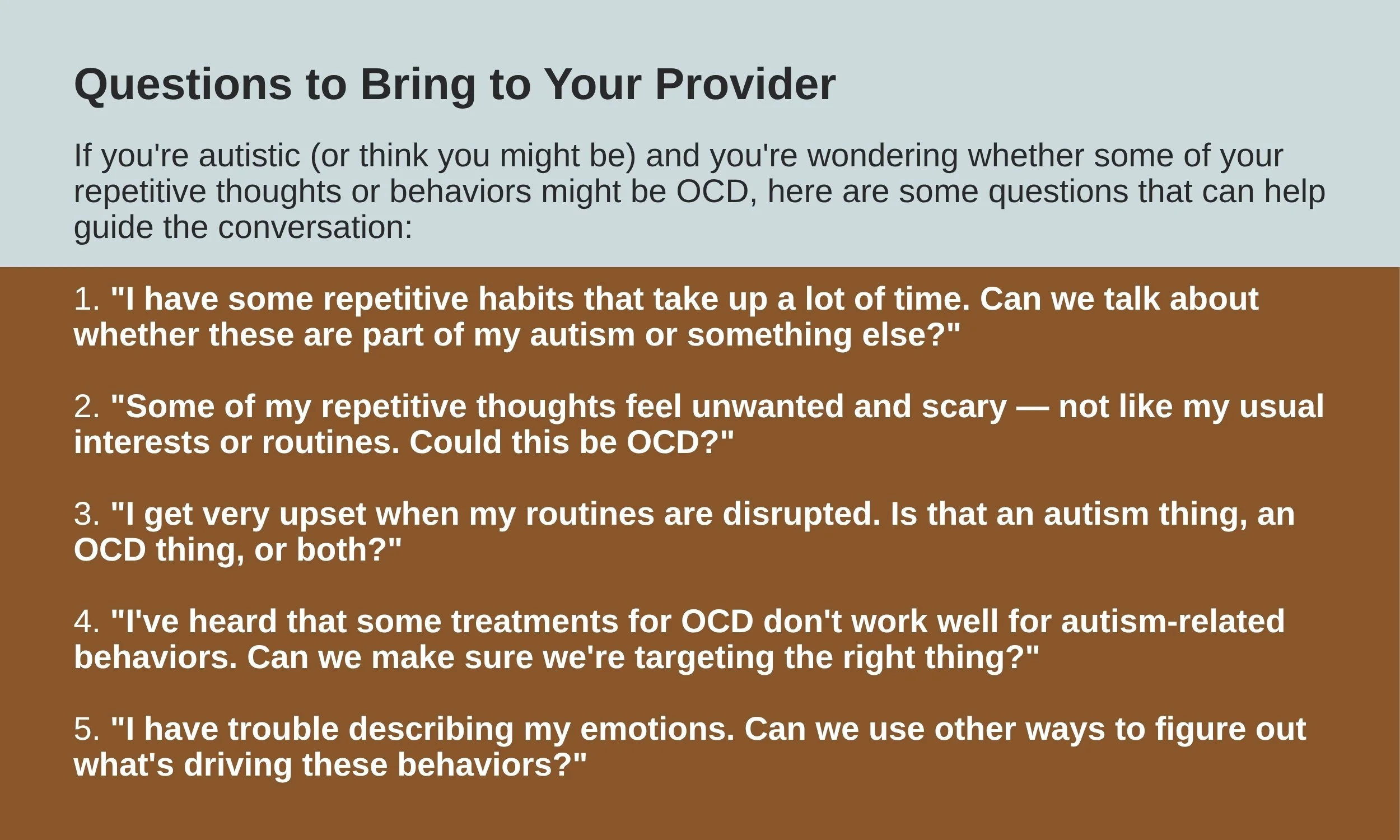
What Should You Do If You Recognize Yourself (or Someone You Love) in These Descriptions?
The most important step is to talk to a healthcare provider who understands both autism and OCD. This distinction cannot be reliably made through self-assessment alone. It requires a careful clinical evaluation that considers:
The history of the behaviors (Were they present in childhood? Did they change over time?)
The function of the behaviors (Are they calming or distressing? Do they serve a purpose?)
The presence of intrusive thoughts (Are there unwanted, frightening thoughts driving the behavior?)
The emotional experience (What happens internally when the behavior is performed — and when it's prevented?)
The broader context (Are there other features of autism present, such as differences in social communication, sensory sensitivities, or a strong need for routine?)
A proper assessment matters because the treatment path depends on the answer:
If the repetitive behaviors are part of autism, the right approach is usually accommodation and support — finding ways to make the behaviors work within daily life, not eliminating them.
If the repetitive behaviors are true OCD, effective treatments exist — including therapy (adapted for autistic individuals when needed) and medication — that can significantly reduce suffering.
If both are present, a provider can help sort out which behaviors to accommodate and which to treat.
The Bottom Line
Not every repetitive thought is an obsession. Not every ritual is a compulsion. For autistic individuals, many repetitive behaviors are a natural and often helpful part of how the brain processes the world — providing structure, predictability, and sensory regulation in an environment that can feel overwhelming.
But sometimes, true OCD does develop alongside autism — and when it does, it deserves to be recognized and treated. The key is understanding the difference: Is this behavior a source of comfort, or a source of suffering? Is it something to accommodate, or something to treat?
Only a qualified healthcare provider can make that determination with confidence. If you see yourself in any of these descriptions, that recognition is a valuable starting point — but the next step is a conversation with someone who can help you understand what's really going on, and what kind of support will actually make a difference.
Do not attempt to self-diagnose or self-treat based on this information. The overlap between these conditions is genuinely complex, and even experienced clinicians find it challenging. What this blog post can do is help you ask better questions — of yourself and of your provider — so that the conversation starts in the right place.